






Physical Bases of Electrosurgery
Electro-surgery is very important in operative endoscopic surgery and probably represents the cheapest way to carry out a section and a coagulation.
Article Information: Publication Date:: 09/01/2005 Update Date:: 09/01/2005
Introduction





Click Images to enlarge
Electro-surgery is very important in operative endoscopic surgery and probably represents the cheapest way to carry out a section and a coagulation.
It is the use of high frequency alternated currents (radiofrequencies) which must increase the temperature within biological tissues in order to obtain different physical effects (section and/or coagulation). Electric power produced by the electro-surgical unit (ESU) is converted, within the biological tissue, into thermal energy. The effects we aim at are determined by a wide range of factors, such as the current exposition time, the electrode shape and size, the way in which energy is applied, etc…
Knowing the physical basis of electrosurgery is mandatory to understand the choice of the instruments, the best way of using them, the methods to avoid complications. Which pedal? should not be heard anymore in our surgical rooms!!


Physical Bases of Electro-surgery
Electrons are energy particles which, by crossing biological tissues, generate heat and, according to the entity of this heating, different surgical effects are obtained.
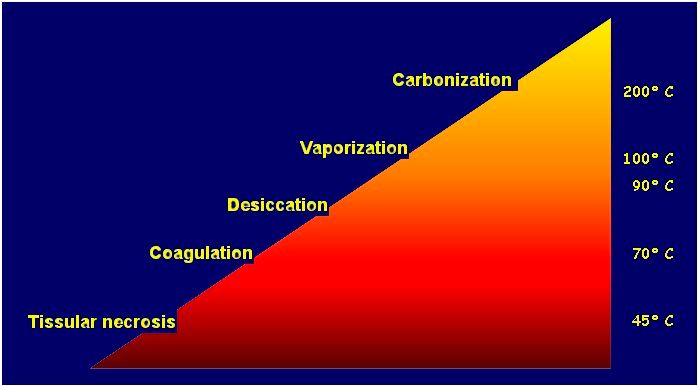
Thermal effects related to different T°
• 37-43° Tissue heating
• 43-45° Retraction
• > 50° Reduction in enzymatic activity
• 45-60° Protein denaturation :coagulation
• 90-100° Tissular dehydration
• >100° H20 ebullition; cell membrane destruction.
• >150° Carbonization
• >300° Vaporization
• >500° Burns


Electricity Properties



The three main properties of electricity are: current (I), voltage (V), impedance (R)
Current is a measure of the passage of electrons in a given point, in a given moment; it is measured in ampere.





In an electric circuit these three properties are expressed by the Ohm law:
I=V/R

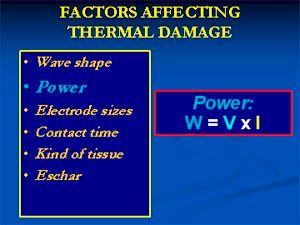
The power (W) is the ability to produce work in time units; it is the energy produced and is measured in watt; it is defined by the product of pressure (volt) x current (ampere). The total energy in a given period is measured in joules.
W=IxV
thus, by replacing I=V/R, we will have W=V x V/R, or rather
W=V2/R
Such relations are fundamentally important to understand some aspects of electro-surgery: for example, at a certain power in watt, the increase in resistance will be accompanied by a strong decrease in voltage; this helps us to understand how, with the same watts, application time, kind of electrode used, the characteristics of cut or clot we obtain with a certain kind of electrode can change.
Definitions of Electrical Terms:
Current: Ampere Volume of Electrons/Sec Flow
Voltage: Volt Strength with which E are pushed
Impedance: Ohm Resistance to Flow
Power: Watt "Work" Produced by E Flow
Energy: Joule "Work" Produced/T


If we compare electricity to hydraulics, an electron could be compared to a water molecule and voltage to water pressure. While water volume is measured in cm3, electron volume, namely its charge, is expressed in coulombs. If we push a volume of water (I) through a pipeline (R), with a certain pressure in a space of time, we would have created a flow of water. In electricity a current, measured in ampere (coulomb/sec), means the passage of a certain amount of electrons through an area in a certain space of time. Both with water and with current, if resistance increases the flow decreases, keeping pressure and/or voltage constant. This resistance which hinders the passage of the electron flow is exactly defined impedance.


Electrical definitions compared to hydraulics
The use of a flow of electrons, pushed through a biological tissue, generates heat and thus a series of thermo-destructive effects, which are the foundation of electro-surgery.

There are two kinds of current:
· directcurrent, characterized only by the variability of its intensity: it is never used in electro-surgery
· alternate current, characterized by its frequency, that is by the number of oscillations per time unit (1 oscillation/sec = 1 Hertz). The frequency used by electro-generators is basic, since the biological effects are also in function of this latter.
We can distinguish
low frequencies from 0 up to 3000 Hz
medium frequencies from 3000 up to 50000 Hz
high frequencies > 50000 Hz.
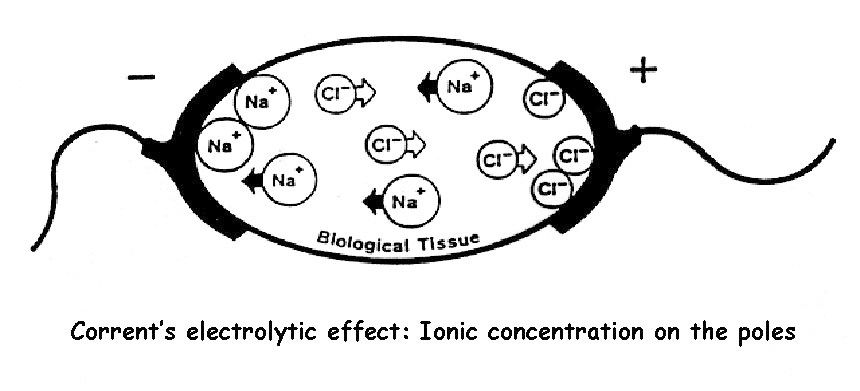
Both low and medium frequencies are no longer used in electro-surgery since, with low frequencies or with direct current, because of an electrolytic-kind effect, sodium hydroxide NaOH and HCl are generated, causing necrosis on biological tissues.


Moreover, frequencies from 0 to 50000 Hz cause negative effects on structures such as muscles and nerves. In fact, the passage of such currents causes neuro-motor excitability phenomena (faradic effect); when such contractions are repeated with a frequency equal to 40 per second we meet a form of complete tetany (fulguration).
The latest electro-generators are machines which produce very high frequency alternate current not stimulating muscular activity, as it happened with the old electro-lancets. With high frequency electric power, the electric flow passage occurs only on the external surface of the crossed structures ("skin effect") without interacting any longer with them at all, but only leading to their heating.



Electro-surgical Generators
Electro-surgical generators are devices capable to convert the normal domestic power, having a frequency of 60 cycles/sec (60 Hertz), into a very high frequency current.
HIGH FREQUENCY CURRENT. BY INCREASING FREQUENCY, THE CURRENT FLOWS MOVES MORE AND MORE TO THE CONDUCTOR’S SURFACE (FARADAY’S LAW, LENTZ’S LAW, MAXWELL’S EQUATIONS). WITH FREQUENCIES HIGHER THAN 100 KHZ, THE PASSAGE EXCLUSIVELY OCCURS AT THE EXTERNAL SURFACE OF THE CROSSED STRUCTURES. (from 500 KHz to 3.0 MHz).
Moreover, they can produce a different-"waved" current in order to obtain different modulations of thermal effects.
Alternate current is characterized by a typical sinusoidal shape, namely with consecutive waves reaching a peak, first in one direction and then in the opposite one.



By means of an oscilloscope we could easily verify that any kind of current has got a "characteristic wave". Such waves are usually symmetrical above and below the base line ("0") thus reflecting the nature of alternate current. The generated peak Voltage is measured by the base line at the wave top.
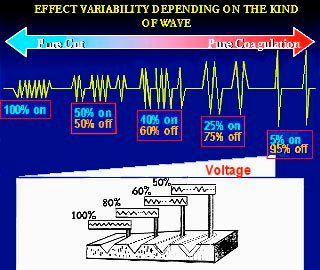
These sinusoidal waves can be interrupted or modulated, leading to different surgical effects.
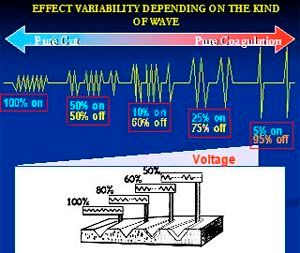
An interrupted sinusoidal wave, whose current is released in pulses (only in 6% of the time, while for the remaining 94% ESU does not release current any longer), forms a coagulation wave. On the contrary, a real wave, a cut one, is an uninterrupted continuous wave; a modulation of these two kinds, with several on-off cycles, is defined mixed or blended current.
A cut current (cut) supplies high frequency current, non interrupted, with low voltage (Vp-p=1000)
A clot current (coag) supplies an interrupted-wave current, with high voltage (Vp-p=6000); in this case the electro-generator supplies power only in 6% of the time (on) while in the remaining 94% the generator does not produce power (off) allowing the electrode cool. These on-off cycles are called duty-cycles.
The high voltages obtained in COAG mode lead to visible voltaic arcs which creates a superficial coagulation, carbonizing the surface, increasing tissular impedance and not allowing the diffusion of the thermal effect in depth. This phenomenon is called Fulguration and the clot current should be used only to obtain this effect, i.e., when there is a diffused, superficial bleeding or oozing.
A blended current is just a continuous cut current which is interrupted by creating several on-off cycles (duty cycles).


For example:
Blend1 means that ESU supplies power only in 80% of the time (on) while in the remaining 6% the generator does not produce current (off) (Vp-p=1200)
Blend2 means that ESU supplies power only in 60% of the time (on) while in the remaining 40% the generator does not produce current (off) (Vp-p=1500)
Blend3 means that ESU supplies power only in 50% of the time (on) while in the remaining 50% the generator does not produce current (off) (Vp-p=2000)
When the current is interrupted, namely when the duty-cycle decreases, the watts are kept constant but the generator increases its voltage (W=VxI) and thus a larger flow of electrons will cross a tissue, with greater side thermal effects, greater haemostat effect but also a greater tissular damage.
Going back to the analogy with hydraulics, this corresponds to the raising of the tower level while the water flow is intermittently blocked at the pipeline end. The higher pressure produced by the raising of the tower causes a higher amount of water flow per time unit.
Alternate Current Effects on a Cell Level:
Cells contain positively charged particles (cations), such as ions Na, K and larger particles, negatively charges (anions), Cl, proteins.
When a radiofrequency alternate current is applied on a biological tissue, it crosses the cells, and because of its effect anions and cations rapidly oscillate in the cytoplasm, raising temperature within the cell. If intra-cell temperature reaches 70-80 °C, protein denaturation will occur and coagulation (white coagulation) will result. If the temperature reaches 90 °C, the cells will lose their water content (dehydration) but will keep their architecture (desiccation).



When the temperature rapidly reaches 100 °C, the water contained in the cells boils; the following formation of vapor and the quick expansion of the intra-cell volume create a cell "explosion", so the cut effect is determined by this vaporization.
When the intra-cell temperature reaches 200 °C, the process defined carbonization occurs.
Electro-surgical Systems
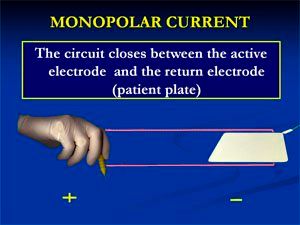
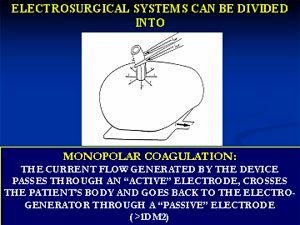
Electro-surgical systems can be divided into two kinds: monopolar and bipolar.
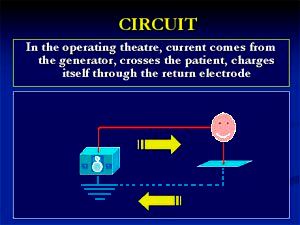
An electric circuit always requires two poles and, in the monopolar mode, the current flow generated by the device passes through an "active" electrode, which can have several shapes and sizes, crosses the patient’s body and returns to the electro-generator through a suitably sized (>1 dm2 ) "passive" electrode which is normally applied on the skin surface.


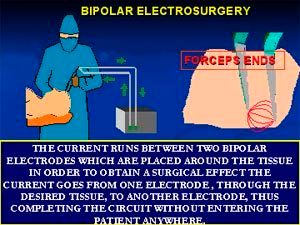
In bipolar mode, the electron flow passes through a forceps jaw, crosses the tissue interposed in the forceps and returns to the electro-generator through the second jaw.



In the monopolar mode, the distance between the two poles can be of many centimetres, so the patient is completely included in the circuit, differently from the bipolar mode where the distance between the two poles (the jaws of the forceps) is usually a few millimetres.



Effects on Tissues of Electro-surgery
The use of electro-surgery in the field of surgery is based on the principle that the human body is a good electric conductor.
Electro-surgery can be used to obtain the tissue section or coagulation.
If vaporization is carried out in a linear way we will get a cut effect accompanied by a coagulation effect along the section line which will be extended in proportion to the used voltage, and, moreover, it will be in function of the speed of the cut execution, of the kind of electrode used, etc..


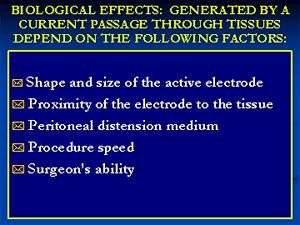
Of course, the biological effects generated by a current passage through biological tissues depend on several factors:



Cut:
The vaporization of a tissue can be obtained by using a monopolar, low voltage, direct current, by using a thin electrode (needle-kind) with a not on contact technique. By this electrode, once the generator has been activated, the current will accumulate at its end, "condensating" and obtaining in this way a high power density. By approaching the electrode’s end to the tissue, without touching it, we will create a voltaic arc between electrode and tissue, by rapidly raising the intra-cell temperature, causing the tissue vaporization. Since the voltage is low and the current is rapidly dissolved and conveyed to the passive electrode (return plate), the side thermal damage will be small.
The level of the side thermal necrosis produced during the cut again depends on many factors: the power, shape and side of the electrode, the wave shape, the voltage peak, the surgeon’s speed and ability. The minimum thermal damage produced and reported in literature is 100 µ even if other studies report 200 µ for the real cut and 300 µ for the blended current.
In theory, using a thin electrode, with a maximum diameter of 1 mm and a 100% duty-cycle current (pure cut output), the power to obtain such effect varies between 30 and 60 watts.
Desiccation and Coagulation
With the word coagulation we often indicate several thermodynamic phenomena where the cell is dehydrated and the proteins are denatured but not destroyed.
When an electrode is put in contact with a tissue, all the energy is transferred to it and changed into heat. Moreover, the electrode shape (usually wider than a cutting needle), with a wider relative area of contact, decreases the power density (the electrons place themselves on a larger surface and do not condensate at the end as on a monopolar needle); in this way the increase in the intra-cell temperature above 100 °C is prevented and a slow evaporation of the intra-cell water is obtained.
Desiccationis the process where temperature reaches 90°C with a consequent dehydration without protein denaturation. We have demonstrated that there is the formation of protein links which create a homogeneous and gelatinoid structure; more or less the same effect produced in hard-boiled eggs. From the clinical point of view, it is difficult to distinguish the two phenomena, so we normally talk about coagulation.

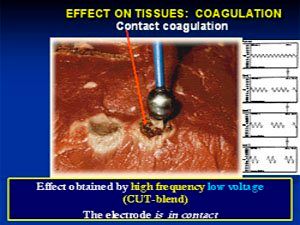


Although we can use all the different "shapes" of electrical waves to obtain a coagulation effect, a real cut current (cut) and/or a blended current (blend 1, 2, 3) should be preferred to the interrupted current (coag). In order to explain this apparent paradox we should take into account that the clot current (interrupted, with high voltage p-p,) causes a huge production of protein links, sometimes preventing the total vase occlusion. Furthermore such currents can lead to an immediate coagulation and dehydration of superficial layers, with a consequent increase in the impedance and, thus, inhibition of the electron passage through the deepest layers. In the end, the "fulguration" effect leads to a quick heating of the tissue accompanied by its adhesion to the electrode. By taking the electrode away from the tissue, also the eschar detaches with a bleeding recommencement.
Thus, coagulation is obtained by using a wide surface electrode, with a real cut or blend current. The coagulation effect is exalted after having obtained a "coaptative coagulation", namely by pressing the haemorrhage source on the tissue itself or by clamping the vase with a grasping forceps. Both these manoeuvres reduce the actual volume of the tissue to coagulate and facilitate the thermodynamic effect, preventing the blood flow, continuing in its run, from removing heat from the energy application site.
Fulguration
Fulguration effect, also known as spray coagulation or black coagulation, is a process where the tissue is superficially carbonized, in consequence of voltage currents (coag), with a very short duty-cycle (6%), applied by means of a wide electrode (sphere-shaped) in no contact mode, that is by keeping the electrode at a few millimetres far from the tissue. The electric arc leads to a quick and sudden raising of tissutal temperature (>200°C).
The electron flow is almost "sprayed" on the tissue so, in this way, the power density is very reduced and the thermo-destructive effect will be diffused but superficial. As mentioned earlier, owing to the superficial nature, there is a quick raising of tissutal impedance, with inhibition of the thermal transfer to the deepest tissues. The practical use of this energy is the coagulation of superficial capillary or arteriole bleedings, more or less extended




A biologically important and clinically fundamental effect is the hyperthermia where the thermal effects are not evident during surgery but occur 48-72 hours later. Cells can survive at temperatures up to 42-45°C but at higher temperatures irreversible damages take place, depending on the reached temperature and on the exposition time to it. The irreversible denaturation of the cytoskeleton proteins is the first event occurring where a temperature of 43°C is applied for 60 minutes. Such thermo-tolerance is approximately halved for each degree of temperature increase. The immediate effects of the energy application are minor and sometimes evident only by means of histochemical investigations or through enzymatic degradation studies. We have reported several cases of intestinal lesions after hysteroscopic surgery (endometrial ablation), with no clear damage of direct lesion.
Variables Changing the Tissue Effects of Electro-surgery

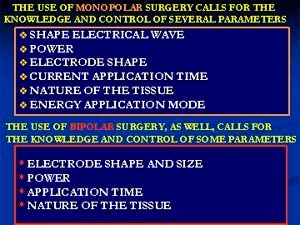
The use of monopolar surgery requires the knowledge and control of several parameters.

The power is difficult to quantify in electro-generators which are not equipped with a digital display; when such devices are not available it is very important to consult conversion tables in order to know exactly how many watts we are using. Power cannot be fixed since it is connected to the electrode size; the thinner it is, the less the power must be to obtain the desired effect.
However, to obtain the same effect we must decrease the power if the tissue is a better conductor and vice versa.
The power in monopolar mode is usually three times higher than in bipolar mode; that is why the bipolar mode’s relative high power and relative low voltage do not allow the power density required to obtain a cut effect.
For example, in monopolar mode, the power required to carry out a coagulation is equal to 50-150 W; in bipolar mode, this value is from 5 to 10 times lower. Generally, the higher the power used (voltage), the greater the strength with which the electrons penetrate into the tissue and, thus, the greater the thermal damage.


The nature of the electric wave. In order to obtain a section and a coagulation, we use electric waves which are different both in frequency and in voltage. The section is carried out with a low voltage (1000-2000 volts), while coagulation uses voltages between 3000 and 9000 volts.
The cut is obtained with a low voltage and a high continuous frequency which lead to a tissue vaporization. The speed of the tissue heating is such as to cause minor damages to the surrounding tissue. The quick raising in the tissue temperature above 100°C leads to the rapid transformation of intra-cell water into vapour with the consequent "explosion" of the cell; thus the heat is dispersed and is not passed on the adjacent cells which remain intact.

The coagulation is obtained with high voltages applied with an intermittent frequency. The coagulation effect increases with the increase in voltage and in the frequency intervals.
The coagulation effect is achieved by means of a progressive cell dehydration; the heat generated by radiofrequencies warms the tissue up to a temperature less than 100°C with the consequent evaporation of intra-cell water and cytoplasm coagulation.
Power density



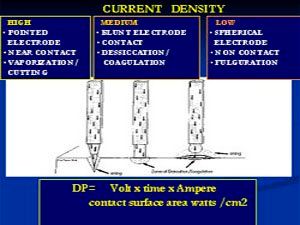
The power density is the total amount of power supplied (in watts) which acts on a tissue for electrode’s area unit (cm2); or it can also be the current amount in contact with the tissue. With the same power supplied, the power density is largely influenced by the electrode shape and size; a thin, needle-shaped electrode will concentrate the electrons at its end, and so a high power density (a high number of electrons) will lead to a quick increase in the intra-cell temperature and to the creation of a vaporization effect of the tissue (cut effect). The same energy, applied by means of a wider electrode (spatula-shaped), in contact with the tissue, will dilute the electron density on its end, thus preventing a quick and sudden temperature raising which will increase more slowly and gradually, obtaining like this a desiccation-coagulation effect. An electrode can be used with a double effect: cut on its sharp side (scissors, spatula) and coagulation on its bevelled surface, which is wider.

The electrode shape is a parameter that surgeons know well. The thinner the electrode, the greater the power density; the wider the electrode, the easier the coagulation effect, as is clear when we use spatula-shaped electrodes. This aspect is exploited when we use curved scissors which lead to a mechanical effect of section and dissection which is associated with a cut or clot effect, determined by whether the scissors thin wall or wide side final electrode is used.
The way in which energy is applied. Without changing the electric parameters, we can obtain effects linked to the way in which we apply the energy. This is extremely clear when we use mixed currents. For example, to perform a section we put the tissue in tension, activate the current and touch the tissue, while to obtain coagulation we do not tighten the tissue, touch it and after that we activate the current. Therefore, the correct technique may be as follows:
In contact: when we establish a contact between the active electrode and the biological tissue and successively we start the electrical contact, the current is immediately dispersed into the tissue.
Not in contact: in this mode, we create a high difference of potential between the active electrode and the tissue, thanks to the air interposition. In this way, we generate an arc (voltaic arc) between the electrode and the tissue surface.
The relation that the active electrode assumes with the target tissue is an important factor: there are two kinds of not-in-contact energetic application:
a) vaporization: the cut effect (vaporization) is a conventional not-in-contact energy application; the formation of an electrical arc from the electrode’s end cuts the tissue, aided by the formation of vapour (vaporized intra-cell water) through which the electrons are easily conveyed and thus obtaining the tissue vaporization. If the electrode is too far from the tissue, the electric arc will not be created and no vaporization will be achieved. On the other hand, if the electrode touches the tissue, there will be a decrease in the power density (since the contact surface becomes wider) creating a desiccation effect, namely a greater thermal damage on the tissues adjacent to the cut line.
b) Fulguration: as before said, using an interrupted, high voltage current, with a short duty-cycle (6%), leads to the "spraying" of the electrons on the target tissue, owing to this strong pressure (high voltage). The distance at which an electric arc can occur depends on the building characteristics of the electro-generator.
When the electrode is kept at a certain distance from the tissue, there will not be any current flow when the generator is activated. We say that the circuit is "open", namely it is interrupted so there is no passage of electricity. In this case, the difference in the voltage produced within the generator is entirely transferred to the electrode. This high "energy content" will be discharged, in the form of an electrical arc, as soon as the distance from the target tissue decreases and allows to "close" the circuit. As far as an "open circuit" is concerned, we should comment on two important things: as already mentioned earlier the electrode acquires a high electric potential (high voltage); it carries much energy which must be diffused very carefully. This situation is potentially very dangerous, especially if we use interrupted current (COAG) since, in this case, the tool induces the greatest capacitive coupling (complications paragraph), reducing the properties of dielectric insulation. Small insulation defects could, under such circumstances, show themselves in thermal lesions due to direct coupling. Consequently any surgeon should remember to keep the "open circuit" time as short as possible.
The other point to note on the use of not-in-contact current concerns the risk of an involuntary thermal damage due to the spark rather than to the current itself. The non-contact effect can be compared to that of a flame-thrower: short interrupted (high voltage) current emissions can lead to the evident "burn" of the superficial layer; however, the lower layer is not thermally damaged; so the impressive apparent damage does not correspond to a depth of the damage itself unlike the contact mode, where all the energy transmitted to the tissue, even at low power, is passed on (by gradient) to the surrounding tissues, causing a deeper tissue necrosis with a modest surface effect, sometimes only a superficial whitening



Tissue impedance: Highly conductive tissues are rich in water thus they offer a scarce resistance to the electricity passage while creating electro-surgical effects. High impedance tissues usually have a low hydro electrolytic content and are relatively bad conductors (bone, fibrous-callous tissue, adipose tissue, electro-desiccated tissues). When we must dissect this kind of tissue, we should change the kind of energy, by increasing the voltage (coag) or by decreasing the duty-cycle (blend current): in this way the current is pushed with a greater strength on low conductibility tissues. Moreover, the impedance is a function of the remainder of the electric circuit and depends on its length, building characteristics, section of electric connections, etc…



Current application time
The amount of energy "administered" to a tissue is directly correlated to the time during which the electrode is kept in contact with the tissue. For example, during an electro-surgical section, if the electrode is slowly moved, there will be a greater side thermal damage. However, if it is moved too fast, a greater thermal damage will result all the same; this happens because, if the electrode touches the tissue, the electric arc will not be created, the power density will decrease and a greater transfer of energy to the adjacent tissues will occur, slowing down the cut effect. Of course, the longer the energy application time, the greater the risks at a distance from the coagulation or cut point .


Peritoneal relaxation medium
The peritoneal relaxation medium should be considered as an integral part of the electric circuit. An electric arc between an electrode and the target tissue occurs only when an interposed electric field becomes strong enough to ionize the interposed medium. These ions collide until the charges given off by the electrode cross the interposed gap and cut on the tissue. Different media have several ionization abilities; for example, CO2 ionizes at 70% while Argon has a better ionization ability and thus facilitates the electrons conductivity (Argon Beam Coagulator).
Bipolar Coagulation
The bipolar coagulation decreases the risks of electrical accident but not the risk of burns of a tissue close to the coagulated area. The two forceps jaws must be well insulated until their active end which closes the circuit when it is clamped on the tissue to coagulate. If we clamp the forceps without any interposition of tissue, the current activation will lead to a circuit with a considerable increase in temperature at the forceps end.
The desiccating effect ("soft coagulation") is the same required for coagulating big vessels (ovarian and uterine ones).
Thus we must take into account and check several factors:
Electrode shape and size. The most common are the Kleppinger, with a good grasping and traction abilities, and the 1 and 3 mm smooth-jaw ones. A thin electrode requires a lower power and leads to a more precise coagulation with a smaller peripheral tissue damage. Since bipolar coagulation enables to reach very high temperatures (up to 340°C) we must take into account that there is a moderate thermal damage until a distance of one centimetre from the forceps. In case of big vessel coagulation (uterine arteries, pelvic-infundibular arteries), the surrounding tissue damage is essential in order to obtain a shutting of the vessel by the simple coagulation.
Power. The absence of electrical risk enables to use high powers. But a high power creates an electric arc between the forceps jaws with consequent carbonization of the tissue which remains adherent to the forceps jaws.
Coagulation duration. A too short application leads to an insufficient coagulation, but a too long coagulation causes an adherence of the tissue to the forceps and an excessive peripheral extension of tissue desiccation.
In order to avoid this problem, the application of an ammeter could be very useful; in fact, when tissue impedance increases owing to the heating underwent by the tissue, the electricity will no longer pass so the ammeter will warn that the tissue desiccation has been "electrically" completed.
This system do not guarantee the completeness of the tissue coagulation but prevents from uselessly continuing a coagulation with a single thermal effect, harmful for the surrounding tissue. After coagulation, the operator will have to perform a cautious section until the appearance of rosy tissue, sign of insufficient desiccation.
Tissue characteristics. Bipolar coagulation causes a remarkable heating of the tissue held by the forceps, and some tissues (i.e., veins) explode, giving an effect opposite to the desired one. In these cases it is necessary to use a lower power and to grip with the forceps a bigger tissue mass.
Electro-surgery complications


Electro-surgery complications follow the thermal trauma and can be classified in two kinds:


A) Thermal damage due to direct coupling
Involuntary and/or accidentally extended activation of the active electrode
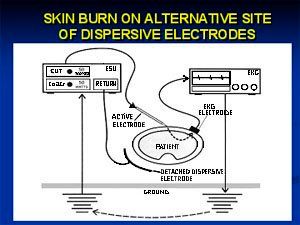
Thermal damage following electrical diversion
- Skin burn on alternative site of earthed electrodes
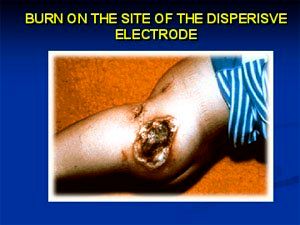
- Skin burn on the site of the earthed electrode (plate)
Burn due to defective insulation of the active electrode
Burn due to accidental contact with non insulated tools
B) Thermal damage due to capacitive coupling
Burn due to electrostatic current discharge
Thermal damage through the active electrode (Mon/Bip)
One of the most common accidents is the unintentional activation of ESU, which can occur when the electrodes are "abandoned" in the abdominal cavity, even when they are not in use and the switch pedal is accidentally activated; it is very important that the electro-generator control is carried out by the surgeon and not by others; in order to prevent this kind of accident, the surgeon should always have the direct control of the generator activation and all the electro-surgical tools should be removed from the peritoneal cavity when they are not used.
When the vaporization/coagulation areas are very close to "noble" structures (ureter, gut, large vessels), the heat transmission, so the thermal damage, could affect these structures; bipolar coagulation can reduce, but not eliminate, this risk. Consequently, the structures to be coagulated and/or sectioned must be anatomically isolated in order to have the chance to apply the most suitable energy.
Thermal damage due to electrical diversion
Electrical diversion can assume several forms: one kind shows itself, for example, when the electrical current finds a different and easier path to leave the patient’s body, compared to the earthed electrode (plate). In this case, if the power density is high enough, thermal damage can occur.
Thermal damage on the level of passive or earthed electrode.
The thermal damage on the level of passive or earthed electrode has nowadays become rare since the modern generators use insulated circuits able to continuously monitor the return current (REM). In the past, even a partial detachment of the plate led to a decrease in its surface and thus to an increase in the power density which generally resulted into burns on the level of the detached plate. In case of an even partial detachment of the plate, the REM-equipped generators block the electricity supply, generally warning with a sound signal. If the generation is not REM-equipped, it is important to carefully control the plate adherence to the skin surface as closer as possible to the intervention site.






Small continue solutions, even macroscopically invisible, of the electrode insulation sheath enable the electricity to go out from such holes, hitting non target structures placed at suitable distance. The high power density which focuses on these small secondary microelectrodes makes them particularly dangerous for the structures in contact with them (gut!!!). This risk is increased by the fact that the surgeon keeps under his/her control only the electrode distal end so the damage normally occurs outside the monitored visual field and is diagnosed too late (peritonitis!).

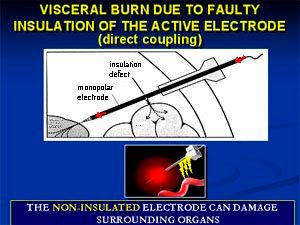


The prevention of these accidents includes a careful maintenance of the electrodes (repeated sterilization cycles in pressure cookers decrease the insulation sheaths dielectric power!) and also a check before using them. A lesion due to direct coupling also occurs when an active electrode involuntarily touches and electrically charges another conductor (optics, cannula, non insulated forceps…) which, in turn, is in contact with a tissue.
Capacitive Coupling
Capacitance is the ability of a conductor in establishing an electric current in a parallel circuit which is not connected to it. When an active electrode is activated, an electromagnetic field creates around it, which becomes a potential capacitor. It is able to transmit a high electrical charge to a parallel and external conductor: the energy transfer (radio waves) occurs from a transmitter (active electrode) to a receiver (conductor metal cannula acting as a receiving aerial) through an insulating medium (air). This phenomenon occurs, for example, when an electrode is inserted through the operational channel of a laparoscope or of a metal cannula.




Normally, when this happens, the current through the metal trocar gets in contact with a wide tissue area and rapidly spreads, going back to the earthed electrode. On the contrary, if the metal trocar is coated with a system of skin anchorage in plastic, the current does not spread through the skin and the laparoscope (or the cannula) becomes a second conductor. By touching a tissue, it discharges the electric amount accumulated with the following thermal effect. This phenomenon is more remarkable if we use high voltage currents (coagulation) with an open circuit.
The prevention of the capacitive coupling phenomenon is carried out by avoiding the use of hybrid (plastic/metal) trocars, using, on the contrary, trocars with anchorage system totally made in metal or totally made in plastic.


A practical rule, simple but effective, is the "3 rule" which consists of the check of the materials in which the tools inserted in the abdominal cavity are made (metal electrodes with possible insulation sheaths, metal or plastic trocars, cannulas, etc…). No more than three different materials must be present simultaneously in order to prevent the risk of capacitive coupling.
The biological effects generated by the use of electro-surgery depend on several factors:
on the kind of tissue crossed (nerves, muscles, fat) and on its impedance
on the kind of current (direct or alternate)
on its frequency
on its intensity
on the ESU electrical power
on the shape and size of the active electrode
on the proximity of the electrode to the tissue
on the peritoneal relaxation medium
on the procedure speed
on the surgeon’s ability
Preventing thermal damages implies respecting the following rules:
to examine carefully the insulating agent of laparoscopic instruments
to use the indispensable minimum powers
to use a low voltage wave (cut)
to prefer intermittent activations rather than prolonged ones
to not supply current into an interrupted circuit
to not activate the electrode close to other instruments
to use bipolar coagulation, when possible
to use metal or plastic trocars, avoiding hybrid systems
to use always the most modern technology
to know in depth the kind of electro-generator
to use the lowest possible power regulation
to not activate the electrode near or in direct contact with metal conductive objects
to extract from the abdomen all the potential active electrodes which are not being used
to keep the best possible visualization of the operating field.
The safety of electro-surgery comes from the understanding
of the basic principles
of the tools
of the effects on tissues
of the areas exposed to thermal damage
of the kind of damages
Glossary
Used energy typology: alternate electrical current
Generator: the machine which converts the low frequency alternate current into high frequency electro-surgical current.
Frequency: number of cycles per second, moving from a fixed point, measured in ampere; used range: 2-3 A.
Voltage: the strength which pushes the electrical current through the resistance;
Used range: 1000-9000 Volt (Monopolar), 300-800 Volt (Bipolar)
Power: the quantity of heat energy produced per second; used range per surgery in dry or wet field: 15 -50 Watt; cut (300 Watt max); Clot (120 Watt max); Bipolar (70 Watt max); (automatic regulation through the instant response or tissue response system).
Functions: real cut, coagulating cut, coagulation, fulguration.
Active electrode: electro-lancet top that we put in contact with the target tissue
Return electrode: plate.
Current density: relation between electrical current flow and crossed surface; current concentration directly proportional to the quantity of generated heat.
Tissue impedance: resistance offered by tissues to the passage of electrical current, measured in Ohm. An obese or very slim individual offers more resistance than a normal built individual.
Coagulation: blood tamponade or destruction of the tissue without cut effect.
Fulguration: it is caused by using electrical arcs (sparks) which jump from the active electrode to the tissue through the air pocket.
Biophysical effects of electro-surgical current
Biological effect: generated by the heat production in the target tissue.
Biotransformation of the target tissue during the cut: Vaporization and consequent expansion of intra-cell water, which leads to the cell explosion (Temp.: 100°C).
Biotransformation of the target tissue during the clot:Protein denaturation (starting at 63°C), desiccation (Temp.: > 100°C), carbonization (Temp.: >150 °C).
Coagulation of arteries with a calibre up to 2 mm.
Potential thermal damage around the target tissue: it can vary from 1-2 mm for cut to 7-8 or more millimetres for coagulation, depending on the power used and on the supply time.
Smoke generation.
Eschar formation.











Advancing obstetric and gynecologic surgery through robotic innovation
April 30th 2024Explore how robotic surgery revolutionizes obstetric and gynecologic procedures, offering enhanced precision, reduced complications, and improved patient outcomes, while also examining challenges and future prospects in the field.
Read More


Unlocking placenta accreta spectrum with single-cell gene targets
April 18th 2024Discover how cutting-edge single-cell RNA sequencing unveils molecular insights into placenta accreta spectrum disorders, potentially revolutionizing diagnostics and treatments for this life-threatening pregnancy complication.
Read More


Excessive gonadotropins in IVF: Effects on mosaicism and live birth
April 12th 2024A recent study revealed a correlation between high doses and prolonged duration of exogenous gonadotropin use during in vitro fertilization and increased embryonic mosaicism alongside diminished live birth rates, prompting reconsideration of dosage and duration protocols.
Read More

Maternal history linked to uterine fibroid risk in Black women
April 11th 2024Delve into the findings of a recent study revealing the heightened risk of developing uterine fibroids among Black women with a maternal history of the condition, shedding light on crucial implications for patient care and advocacy.
Read More

