






The importance of Visual Port Insertion During Laparoscopy
Patient safety is finally being institutionalized due to growing concern over the terrible cost of inadvertent human error. Medicine's punitive perfectibility model in dealing with unintended injury is slowly evolving to accept error during surgery, as an inevitable yet manageable reality of operations (Leap, 1994).
Reprinted with kind permission from TheTrocar.com
Introduction
Patient safety is finally being institutionalized due to growing concern over the terrible cost of inadvertent human error. Medicine's punitive perfectibility model in dealing with unintended injury is slowly evolving to accept error during surgery, as an inevitable yet manageable reality of operations (Leap, 1994).
The White House Advisory Commission report on Consumer Protection & Quality in the Health Care Industry identified medical error prevention as an important issue in Health-Management. Congress passed legislation ordering the Agency for Health Care policy and Research, to identify strategies, to reduce medical error in all fields where "human error" may lead to irreparable injury.
Laparoscopic surgery presents a unique and intricate safety challenge, compared to conventional surgery, as it is a more demanding specialty with technology dependent complex applications with poor redundancy.
Even with considerable technologic innovations in endoscopy, little has changed in our understanding of port dynamics, and accident causation. Consequently, half of serious laparoscopic complications continue to be access related, and many bowel injuries go undetected.
Laparoscopists are expected to perform flawlessly, in a distorted proprioceptive environment, where depth perception, tactile feedback and other important intuitive fundamentals of conventional surgery are lacking. Surgeons are aware of these potential dangers during surgery, especially those associated with laparoscopic Primary port creation using conventional blind push-through sharp trocar methods ( Hashizume and Sugimachi, 1997; MacCordik et al, 1999; Nuzzo et al, 1997).
Fortunately, the incidence of serious laparoscopic injury is rare. A recent Physician Insurers Association of America white paper on worldwide access injury statistics and compensation trends indicate, that the number of laparoscopic injury claims and amount of indemnity paid has significantly increased over the last five years. Between 1990-94, 750 laparoscopic claims were closed costing $ 42,271.068, however, between 1995-99, of 1426 claims, $104 million was paid with a higher mean compensation value (Bartholomew et al, 2000).
In a large prospective study by Jansen, there was an overall complication rate of 5.7/1000 laparoscopic procedures (Jansen et al, 1997). It is acknowledged that access injury accounts for up to half the incidence of reported serious laparoscopic complications (Deziel, 1994; Chandler and Bartholomew, 1997).
The increasing number of procedures performed globally, growing laparoscopic applications in different surgical fields, an increasing frequency of repeat laparoscopies performed on the same patients, with an ever increasing frequency and size of awards, necessitate serious study of accident causation and urgent redesign of our access methods.
The Medical Device Reports (FOI Services Inc, Gaithersburg, Maryland) data has registered more than 400 serious laparoscopic injuries and 20 deaths for the period between 1994 to 1997, related directly to conventional push-through blind access trocars. Furthermore, laparoscopic mishaps are now less tolerated and most injuries proceed to litigation with attempt at financial compensation (Garry, 1999).
Given our present knowledge and technology, absolute prevention of technical misadventures, while desirable medico-legally, may be clinically unachievable. Evidently, technical limitation and unavoidable surgical complications are part of the laparoscopic approach ( Kern, 1997).
Access systems that use a trocar and cannula design have been described as First Generation, as they require application of perpendicular Penetration Force at port site, through a sharp or pointed trocar, so as to propel the trajectory blindly into a body cavity. These methods fail to demonstrate and archive port dynamics during insertion and port removal. Consequently error is not registered, and cannot be recalled.
Conventional push through blind trocar systems fail to provide any access redundancy, where an interactive, real time and error tolerant access environment can anticipated, avoided or at the very least recognized error when injury occurs (Ternamian, 1999).
Our ability to introduce safer port methods and intuitive access designs has been limited, as most conventional First Generation trocar and cannula access systems are blind. Investigators have been unable to objectively analyze and appreciate tissue dynamics at port site. Most serious access injuries are conveniently assigned to human error with very little error analysis and no injury causation studies. As a result little significant change has occurred in our understanding of port safety, competence, and port toilet.
In order to prevent error recurrence and introduce a laparoscopic port creation system that allows error recovery, detailed Failure Analysis has to be conducted (Troidl et al, 1993). To understand this process, three steps have to be undertaken. First, is analysis of incident reports and published frequency of complications. Second, is critical analysis of error dynamics. And third is introduction of innovative system changes that allows archiving of port dynamics, in real time, so that we may be able to eventually understand error (Troidl et al, 1991).
Detailed observational studies are required to identify weaknesses of surgical methods to help determine specific Performance Shaping Factors (PSF) that underlie laparoscopic port accidents and contribute to surgical complications (Joice et al, 1998).
Conventional push-through trocar and cannula design access systems require application of considerable axial Penetration Force to a sharp or pointed trocar. Insertion of the trajectory is usually blind and uncontrolled where the anterior abdominal wall is tented towards the viscera.



Compilation of these increments of access danger PSFs, during port insertion, renders the process more error-prone and sets the stage for inadvertent injury, an accident waiting to happen. Accessing becomes a perilous first step during laparoscopy, even in the best-trained hands, using contemporary instruments and methods (Ternamian, 1997). In a large Finnish study, risk of entry-related injury was higher in operative compared to diagnostic laparoscopy (Hrkki-Siren et al, 1999).
Surgeons are often reminded that most serious access injuries are operator error-related, implying that inexperience, lack of surgical judgment or failure to adhere to strict insertion techniques are the principal causative factors (Marret et al, 1998; Chapron et al, 1997). However, in complex safety-critical domains other than health, where error prone tasks are performed by a team of humans, it is proven that punishment of individuals, training, and motivation, is an ineffective means of preventing further adverse events (Reason, 1992).
Probably, rather than instigating accidents; endoscopists are victims of unreasonable patient expectations, poor access system design and sub-optimal instrument ergonomics. This significant shift from "blaming the human", allows surgeons to reexamine taxonomy of port insertion, appreciate importance of access redundancy, archiving and recall. Then one can understand port competence issues, and appreciate that port insertion and removal is more complex than previously accepted.
Second Generation Visual Port System: ENDOTIP™
The Second Generation laparoscopic port insertion system is developed to buffer error, through system redesign and ergonomic instrument change to avoid incorporation of previously identified PSFs.
It is accepted that trocar entry lacerations can be considerably reduced if port insertion is visual (Marret et al, 1997; Mettler et al, 1997).
A port system to be truly interactive, it must incorporate an error anticipation feature, where the image capture mechanism visualizes port tissue-dynamics, as it evolves in real-time, ahead of the advancing cannula. Visual control, is an important safety ingredient during laparoscopic ancillary port placement as well. The importance of visual port removal is also recognized, as it relates to long-term port competence and port contamination issues.
In this article, the visual laparoscopic Second Generation access system called ENDOTIP™ is described and its different applications illustrated, that by design renders port creation more redundant and forgiving.
Instrument Design
The Endoscopic Threaded Imaging Port ENDOTIP™ has a proximal valve section and a distal stainless steel



cannula section with a single thread winding diagonally on its outer surface. The thread ends distally in a blunt end. It is available in several lengths and diameters for different surgical applications. It may be used at primary or ancillary port and can be applied during closed or open laparoscopy. This reusable cannula allows extra- or retro-peritoneal laparoscopic operations (Ternamian, 1998).
A plastic locking ring (telescope stopper), is mounted ahead of the cannula onto a zero degree laparoscope, to keep the monitor picture in focus during port creation. The reusable ring comes in different sizes, to fit telescopes of different diameters.
Surgical Technique
When performing sophisticated endoscopic operations, surgeons must be versed in conventional open surgeries well as the laparoscopic approach. The decision to pre-insufflate (closed laparoscopy) or apply the primary port first and then insufflate will depend on the surgeon's training and other clinical considerations.
An umbilical skin incision is made with a 15mm round-tipped surgical blade, to allow the cannula into the wound. Ribbon retractors and peanut sponges are used to expose the anterior rectus fascia. A small 8 mm anterior rectus fascial incision is then made under direct vision.
ENDOTIP Cannula Insertion At Primary Port During Closed Laparoscopy
The Veress needle is inserted through the small anterior fascial incision in the usual way. During insufflation, a 0° laparoscope is defogged and camera white-balanced, then the telescope stopper followed by cannula are mounted. The telescope stopper is locked to keep the laparoscope 2cm short of the cannula's distal end.
The camera is focused to the cannula's blunt end and laparoscope is held vertical to the patient's supine abdomen using the surgeon's non-dominant hand.
When the insufflation is complete, the Veress needle is removed, and cannula lowered into the umbilical well, with the CO2 stopcock in the closed position. The cannula is rotated clockwise, using wrist muscles of the dominant hand, while keeping the forearm horizontal to patient's abdomen with the surgeon's shoulders square in resting position facing the monitor.


Further rotation of ENDOTIP™ will part the peritoneum incrementally, under direct visual control, without use of pointed or sharp trocars and without applying perpendicular penetration force. It is important to keep the cannula perpendicular to the tissues at all times, to avoid tunneling.
When the pre-peritoneal layer is reached, if intra-peritoneal adhesions are present, the intense light ray of the laparoscope is reflected off the adherent scar tissue and the area looks white instead of the typical translucent grayish-blue. Most post-surgical parietal peritoneal adhesions are linear and tissue hangs vertically in the insufflated abdominal cavity. Surgeons often find a clear grayish-blue adhesion-free segment, through which entry is safely achieved .



The cannula is lifted slightly to disengage the cannula's blunt end and free rotated to a clear sector under visual control, where the end is re-engaged by clockwise rotation, to part the peritoneal membrane, starting from an adhesion-free clear sector. During clockwise rotation, adherent tissues tend to move radially out of harm's way, allowing safe and visual placement of primary cannula past adhesions.
ENDOTIP Cannula Insertion At Primary Port During Open Laparoscopy
When inserting ENDOTIP™ at primary port without pre-insufflation, infiltrate the umbilical and subcutaneous area with 5ml of Marcaine ¼ % and 1/200,000 Adrenaline. Using a 15mm surgical blade, a skin incision is made and subcutaneous tissue meticulously dissected to expose the anterior rectus fascia


The laparoscope is defogged and camera white-balanced. Then the telescope stopper followed by the cannula are mounted. The telescope stopper is then locked to keep the laparoscope's end 2cm short of the cannula's distal end. The camera is focused to cannula's blunt end and laparoscope is held vertical to the patient's supine abdomen using the surgeon's non-dominant hand.
ENDOTIP™, with CO2 stopcock in open position, is then lowered into the umbilical well, and rotated clockwise using the wrist muscles of the dominant hand, while keeping the forearm horizontal and shoulders square in resting position.
ENDOTIP™ engages the anterior fascial window, parts radially, and then lifts to transpose successive tissue layers on to cannula's outer thread. The white anterior rectus fascia, red rectus muscle, then pearly white posterior fascia, are pulled up along the outer pitch, until the yellowish pre-peritoneum.
At this level, given the intense light and magnification of the laparoscope, bowel peristalsis or omentum may be observed on the monitor, across the transparent peritoneal membrane, moving with the respiratory movements of the patient. Once a peritoneal opening is created, room-air streams through the cannula's open CO2 stopcock, into an airless peritoneal cavity.




Free peritoneal fluid or blood when present intra peritoneally, is seen to pool into the cannula, partly obstructing visualization. Once CO2 insufflation is initiated, the rising abdominal wall drains the pooled fluid back into the cavity.
During retro- or extra-peritoneal laparoscopic procedures, such as para-aortic lymph node dissection, TEP or uro-suspension procedures, the cannula's rotation is stopped once the desired tissue layer is reached. A virtual cavity is then created under direct vision by blunt dissection with the laparoscope and CO2 insufflation at low pressures, <5mm Hg. As dissection is visually monitored, inadvertent perforation of the peritoneal membrane is avoided.
At ancillary ports especially, where the skin incision is small, ENDOTIP™ anchors securely at port site by the outer thread. This snug fit discourages CO2 loss. Several onco- and uro-laparoscopists, prefer the retro peritoneal approach as it is thought to cause less pain and less risk for bowel or vascular injury (Kuenkel et al, 1993).
Although safe to be used in any body weight, overweight patients and those who have had previous abdominal surgery could require longer instruments and insertion time (Ternamian and Deitel, 1999).
ENDOTIP Cannula Insertion At Ancillary Port
During ancillary port insertion, a skin incision and dissection of subcutaneous tissue using the scalpel's handle is all that is needed; an anterior rectus fascial incision and ancillary telescope is not necessary. As with all ancillary port insertions, ENDOTIP™ must also be introduced under direct visual control through the primary port.




The course of the superficial epigastric and inferior epigastric vessels must be determined prior to insertion. The urinary bladder must always be emptied before inserting a suprapubic port. If the obliterated umbilical


artery is encountered, a peritoneal opening can be created using an L-hook cautery through the partly inserted ancillary port. The cannula is then threaded through the peritoneal opening.
ENDOTIP Cannula Removal
When the operation ends, CO2 stopcock is closed, tubing is disconnected, laparoscope retracted 2cm into the cannula, telescope stopper is locked in position, and camera is focused to cannula's end. The laparoscope is held perpendicular to patient's abdomen with the non-dominant hand, and cannula is rotated counterclockwise with the surgeon's dominant hand.
CO2 is released through an ancillary cannula to avoid spraying of body fluids onto telescope's lens. The anterior abdominal wall layers disengage in sequence off cannula's outer thread, to regain its natural grid-iron orientation and restore shutter mechanism at access site.
The threaded cannula is gradually rotated counterclockwise, with the laparoscope mounted, until it is completely removed. Removal is visual, incremental and controlled. Tissue injury or entrapment along cannula's path is avoided.
Rapid cannula removal is discouraged, instead surgeons can visually identify compromised or at-risk port sites and take appropriate measures to reinforce fascia to avoid hernia formation, although port-site fascial closure does not necessarily avoid hernia formation (Montz et al, 1994).
Closure of fascial defects is important when cannulas with a diameter of >10mm are used, when fascia at port-site is extended for surgical tissue retrieval, when port-site tissues are inflamed or very thin, when infection is suspected, when the patient has chronic cough or asthma, following long laparoscopic operations, and when tissue integrity seems compromised.
Conclusion
Creation of ports has always been considered a critical first step in laparoscopy. Over the years, several authors have suggested newer port devices to improve safety, with no real change in the conventional push-through trocar design or access system.
First generation port systems require considerable, uncontrolled axial Penetration Force at port-site to thrust the trajectory blindly towards the peritoneum. This access system is unable to anticipate, avoid or recognize error when mishaps occurs, and has no error redundancy.
A new Second Generation port system and reusable access instrument is described to render laparoscopic port insertion and removal error-tolerant. The ENDOTIP™ system effectively buffers inevitable surgical error, through access system redesign where perpendicular Penetration Force is avoided by realigning direction of entry force from axial to radial. Sharp or pointed trocars are not required, and visual, incremental and interactive port creation is possible. It allows the surgeon to navigate past vessels, bowel or adhesions.
Moreover, this access system visualizes and archives port dynamics and incorporates several intuitive safety features that captures error in real-time, when and if mishaps occur, and offers the surgeon an error-recovery opportunity to avoid error-progression to serious patient harm.
By recording and reviewing our access and exit methods in real-time, surgeons can analysis port dynamics and understand better error causation. A timely error recovery opportunity, can prevents error from progressing to permanent harm. In addition, one may also have an opportunity to better appreciate port toilet and port competence concerns.
Rather than blaming individual surgical performance or specific instrument design, introducing tolerant laparoscopic access system changes, with different levels of redundancy, will improve patient safety and reduce the probability of recurrent error.
With Congress aiming at a fifty percent reduction of unintended medical error over the coming five years, patient safety initiatives such as safer laparoscopic access methods and instruments are urgently needed to render Minimally Invasive Surgery a truly patient friendly and less dangerous operative method.
References:
Correspondence: Dr. A.Ternamian, 77 Truman Road, Toronto, Ontario, M2L 2L7 CANADA.
e-mail: artin@pathcom.com
Presented in part at the10th Congress of the European Society for Gynecological Endoscopy, Lisbon. November 2001
References
1. Bartholomew L, Traywick R, Quinn R, Scalettar R, Stanchfield J. Laparoscopic Injury Study. "Insuring the Practice of Quality Healthcare" Physician Insurers Association of America 2000
2. Chandler J, Bartholomew L. Complications of cholecystectomy. J of Gastrointestinal Surg 1997; 1: 138-145.
3. Chapron C M, Pierre F, Lacroix S, et al. Major vascular injuries during gynecologic laparoscopy. J Am Coll Surg 1997; 185: 461-465.
4. Deziel DJ. Avoiding laparoscopic complications. Int Surg 1994; 79:1-4. (Medline)
5. Garry R. Towards evidence-based laparoscopic entry techniques: clinical problems and dilemmas- Editorial. Gynecol Endosc 1999; 8: 315-326.
6. Härkki-Sirén P, Sjöberg J, Kurki T. Major complications of laparoscopy: a follow-up Finnishstudy. Obstet Gynecol 1999; 94: 94-98. (Medline)
7. Hashizume M, Sugimachi K. Needle and trocar injury during laparoscopic surgery in Japan. Studygroup of endoscopic surgery in Kyushu, Japan. Surg Endosc 1997; 11: 1198-1201. (Medline)
8. Jansen FW, Kapiteyn K, Trimbos-Kemper T, et al. Complications of laparoscopy: a prospectivemulticentre observational study. Br J Obstet Gynaecol 1997; 104:595-600. (Medline)
9. Joice P, Hanna GB, Cuschieri A. Errors enacted during laparoscopic surgery-a human reliabilityanalysis. Applied Ergonomics 1998; 29: 409-14. (Medline)
10. Kern KA. Malpractice litigation involving laparoscopic cholecystectomy. Cost, cause, andconsequences. Archiv Surg 1997; 132: 392-398. (Medline)
11. Kuenkel M, Schaller G, Korth K. Retroperitoneoscopy-the approach to urological minimal invasive surgery. J Endouro 1993; 7: (Suppl 1): S224.
12. Leap L.L. Error in medicine. Special Communication. JAMA 1994; 272: 1851-1857.
13. Mac Cordick C, Lecuru F, Rizk E, et al. Morbidity in laparoscopic gynecological surgery. Surg Endosc 1999; 13: 57-61. (Medline)
14. Marret H, Pierre F, Chapron C, et al. Complications of laparoscopy caused by trocars. Preliminary study from the national registry of the French Society of Gynaecologic Endoscopy. J Gynécol Obstét Biol Repro 1997; 26: 405-412. (Medline)
15. Marret H, Harchaoui Y, Chapron C, et al. Trocar injuries during laparoscopic gynaecological surgery. Report from the French Society of Gynaecological Laparoscopy. Gynecol Endosc 1998; 7: 235-241.
16. Mettler L, Ibrahim M, Vinh VQ, Jonat W. Clinical experience with an optical access trocar in gynecological laparoscopy-pelviscopy. J Soc Laparoend Surg 1997; 1: 315-318. (Medline)
17. Montz FJ, Holschneider CH, Munro MG. Incisional hernia following laparoscopy: a Survey of the American Association of Gynecological Laparoscopists. Obstet Gynecol 1994; 84: 881-884. (Medline)
18. Nuzzo G, Giuliante F, Tebala G D, et al. Routine use of open technique in laparoscopic operations. J Am Coll Surg 1997; 184: 58-62. (Medline)
19. Reason J. Human Error. Cambridge, Mass: Cambridge University Press; 1992.
20. Ternamian A. Laparoscopy without trocars. Surg Endosc 1997; 11: 815-818. (Medline)
21. Ternamian A. A trocarless reusable visual-access cannula for safer laparoscopy; An update. J Am Assoc Gynecol Laparosc 1998; 5: 197-201. (Medline)
22. Ternamian A. A 2nd generation laparoscopic port system: EndoTIPâ¢. Gynecol Endosc 1999; 8:397-401.
23. Ternamian A, Deitel M. Endoscopic Threaded Imaging Port (EndoTIP) for laparoscopy: Experience with different body weights. Obes Surg 1999; 9: 44-47. (Medline)
24. Troidl H, Eypasch E, Spangenberger W, et al. Schonendes Operieren. Verfahrenswahl und Strategie. Invasives versus minimal invasives Operieren. Langenbeck Arch Chir Suppl 1991: 48.
25. Troidl H, Bäcker B,Langer B, et al. Fehleranalyse-Evaluierung und Verhütung von Komplikationen; ihre juristische Implikation. Langenbeck Arch Chir Suppl 1993: 59-72.
Legend for Figures
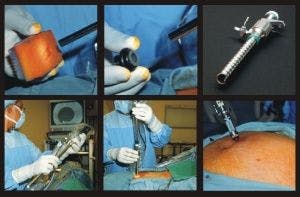
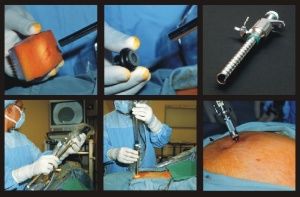
Fig 1 - First Generation access system. Conventional push through blind sharp trocar and cannula.
Fig 2 - Second Generation access system. ENDOTIP⢠Cannula and Telescope Stopper. (KARL STORZ, Tuttlingen, Germany)
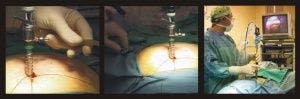
Fig 3 - During insufflation camera is white-balanced, laparoscope defogged, and mounted into the ENDOTIP⢠cannula.
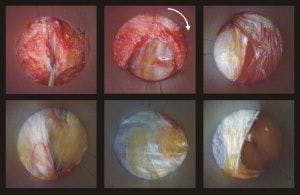
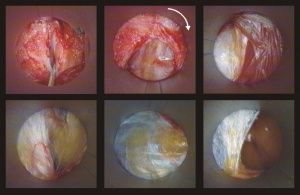
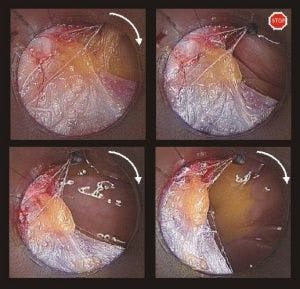
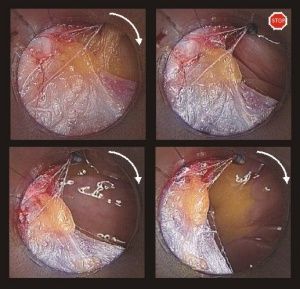
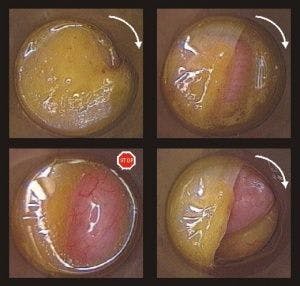
Fig 4 - ENDOTIP⢠cannula insertion at Primary port during Closed laparoscopy. (CO2 stopcock in closed position) Clockwise rotation lifts, white anterior rectus fascia (AF), red rectus muscle (M), then pearly-white posterior fascia (PF) up along outer thread until yellowish pre-peritoneal space (PS)is reached. CO2 filled, adhesion-free peritoneal cavity looks grayish-blue in color.
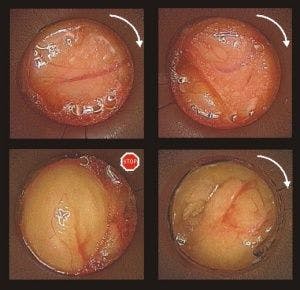
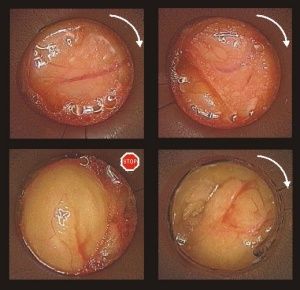
Fig 5 - ENDOTIP⢠cannula insertion at Primary port during Open laparoscopy. (CO2 stopcock in open position) Anterior rectus fascia incised with 15 mm scalpel. Blunt cannula tip (T) White anterior rectus fascia (AF), red rectus muscle (RM), then pearly-white posterior fascia (PF) are pulled up along outer thread until yellowish pre-peritoneal space is reached. Pre-peritoneal space (PS).
Fig 6 - When peritoneal cavity is entered, rotation is stopped and insufflation initiated under visual control. When presenting organ is retro- or extra-peritoneal, such as large bowel (LB), air streams underneath peritoneal membrane (PM), peritoneal edge is clearly seen.
Fig 7 - When presenting organ is freely mobile in peritoneal cavity, such as small bowel (SB), once peritoneal cavity is entered, room-air streams in through open CO2 stopcock. Small bowel balloons into cannula. Rotation is stopped and insufflation initiated under visual control.
Fig 8 - Once peritoneal layer is reached, thin peritoneal membrane transilluminates. Omentum or bowel is recognized and inadvertent injury avoided. When a peritoneal opening (PO) is created, room air streams in through open CO2 stopcock. Omentum (O) will balloon into cannula. Rotation is stopped, and insufflation is initiated under vision. Omentum falls back into peritoneal cavity. Clockwise rotation is resumed to complete insertion.
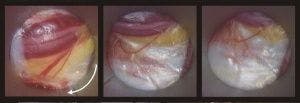
Fig 9 - Vessels encountered along cannula's tract are not transected, they are not transected, they are deflected radially out of cannula's path.
Fig 10 - Anterior abdominal wall layers disengage is sequence off cannula's outer thread to regain natural grid- iron orientation and restore shutter mechanism at access site. Peritoneum (P), Posterior rectus fascia (PF), Rectus muscle (M), Cannula tip (T), Anterior rectus fascia (AF).











Advancing obstetric and gynecologic surgery through robotic innovation
April 30th 2024Explore how robotic surgery revolutionizes obstetric and gynecologic procedures, offering enhanced precision, reduced complications, and improved patient outcomes, while also examining challenges and future prospects in the field.
Read More


Unlocking placenta accreta spectrum with single-cell gene targets
April 18th 2024Discover how cutting-edge single-cell RNA sequencing unveils molecular insights into placenta accreta spectrum disorders, potentially revolutionizing diagnostics and treatments for this life-threatening pregnancy complication.
Read More


Excessive gonadotropins in IVF: Effects on mosaicism and live birth
April 12th 2024A recent study revealed a correlation between high doses and prolonged duration of exogenous gonadotropin use during in vitro fertilization and increased embryonic mosaicism alongside diminished live birth rates, prompting reconsideration of dosage and duration protocols.
Read More

Maternal history linked to uterine fibroid risk in Black women
April 11th 2024Delve into the findings of a recent study revealing the heightened risk of developing uterine fibroids among Black women with a maternal history of the condition, shedding light on crucial implications for patient care and advocacy.
Read More

